ART Orthodontics: Your Best Choice for Orthodontic Braces and Invisalign in Davie Florida
Orthodontic treatment involves attaching brackets (braces) and wires or Invisalign and attachments to teeth – but how do they move teeth? Here I explain the components of braces and clear aligners (e.g. Invisalign and Sure Smile) and the biological principles involved in tooth movement.
If you find the below information useful and are interested in coming to ART Orthodontics for an orthodontics consultation, please click the link below to book your complimentary consultation online.
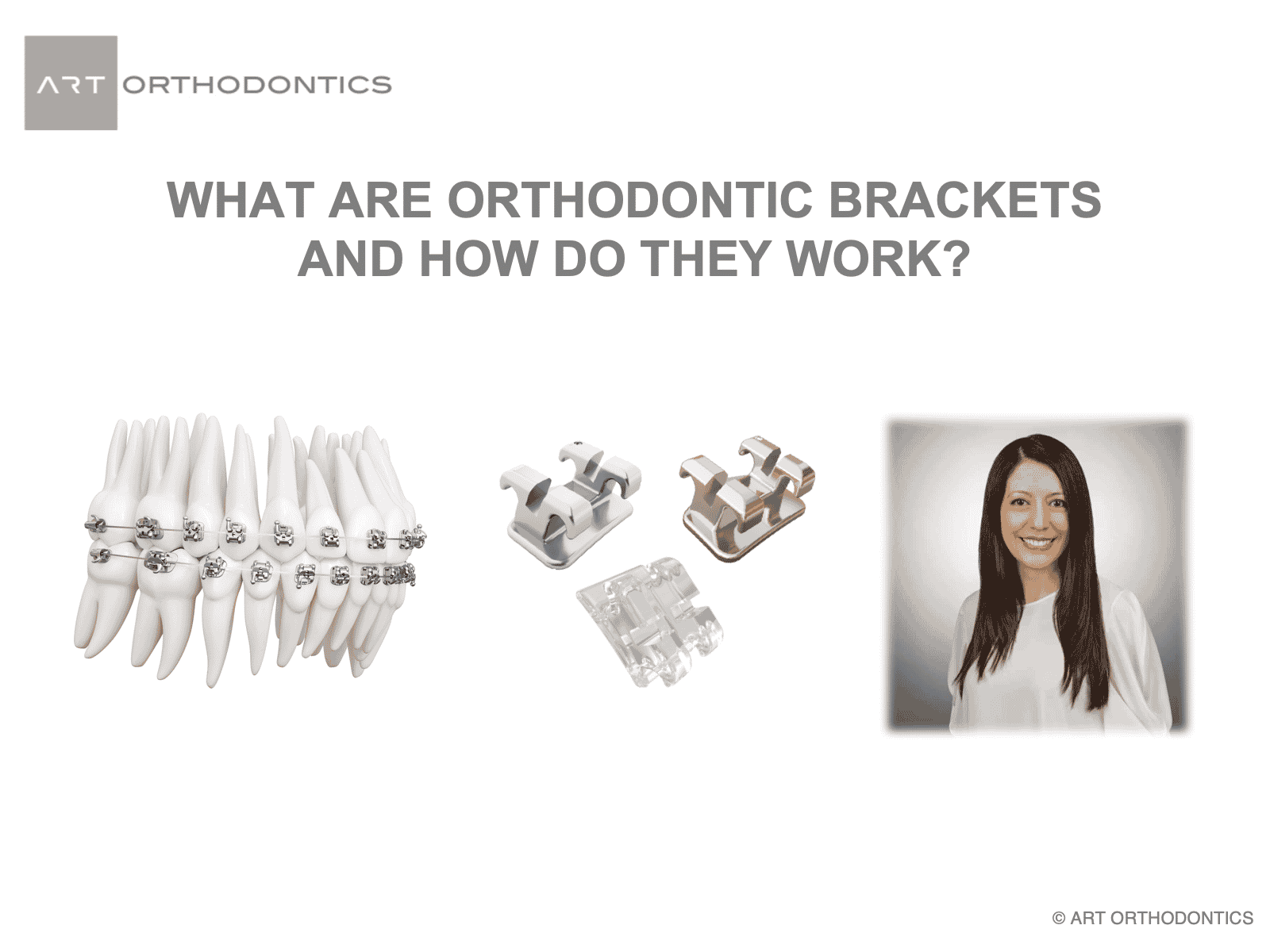
Here are three general bracket types. A tube bracket – on the left. A twin bracket in the middle. A self-ligation bracket on the right.
Orthodontic brackets have different components including a “slot” to hold the wires and “wings” and “hooks” to hold ties or other attachments such as elastics. The ends of archwires pass through and are held in place in orthodontic “tubes”.
The tube bracket holds the wire after the wire is inserted. Tube brackets are generally used for the back teeth since the molar teeth are difficult to access and there are heavy bite forces. With a tube bracket no extra tying in of the wire is needed and the wire is held in place firmly after it is inserted.
Conversely, twin brackets support the wire in their slots with little elastics wraps around the wings to hold the wire in place. Those are the colorful ties that you choose every time you come in for adjustment visits!
Self ligation brackets have built-in “ties” in the form of a gate. When the gate is closed, the wire is held in place.
During the adjustment (tightening) visit, your orthodontist decides if a different shape, size, or material of archwires should be inserted into the brackets or the elastics are re-tied like your shoelaces to allow certain movements happen in your teeth. Sometimes, your orthodontist makes some bends in the archwires to move certain teeth in different directions. Gaps may be closed with use of “powerchains” which are elastic ties that are attached together. Gaps may be opened up with use of coil springs to create spaces around narrow teeth for reshaping by your restorative dentist. You may be advised to wear elastics that hook on your teeth in different areas and directions to help align your bite.
This picture shows the colors that can be added to the braces and the difference to self-ligation braces.
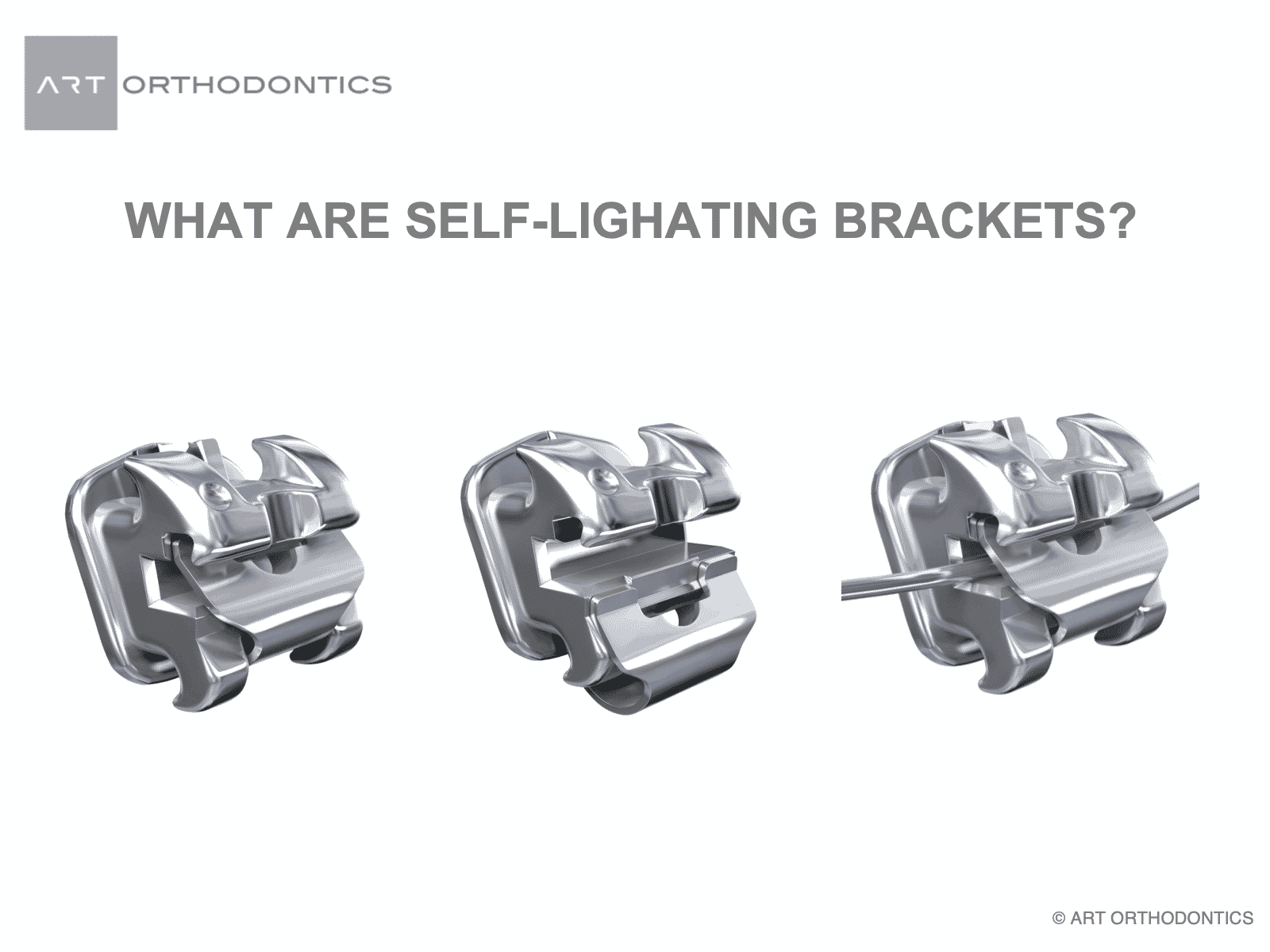
Self-ligating brackets have “gates” to cover the front of the slot. This minimizes friction of the wire with brackets as teeth slide along the wires and therefore makes tooth movement more efficient. Since there is no need to change the elastic ties, your adjustment intervals can be extended to 6-8 weeks. This reduces the number of visits to your orthodontist office since there is no need to change the old worn out discolored rubber ties!
The self ligating brace and the gate that is closed on the left and open in the middle and the gate locking the wire in place on the right.
Self ligation brackets don’t need to be tightened in the traditional way that twin braces are. Self ligation braces are only tightened when a new larger wire is used or when a bend is required in the archwire to move certain teeth in specific directions.
Generally with self ligation braces, patients do not have to come as often to have their braces tightened. Also, without the color ties around each brace, the braces are easier to keep clean. Another nice feature of self ligation is gentler forces on the teeth and less discomfort of having the braces tightened every month.
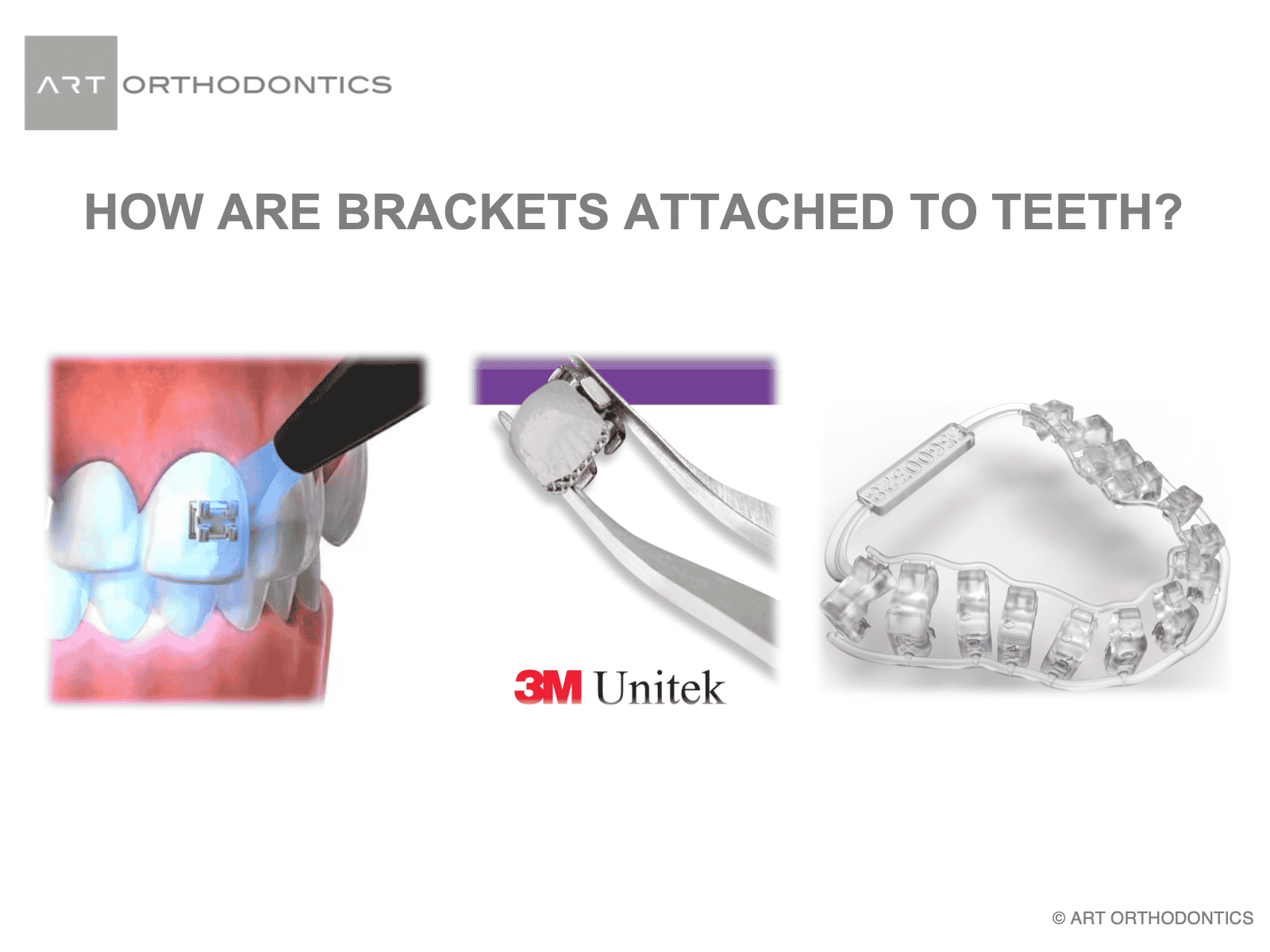
Braces are glued or bonded to the teeth. This can be done directly by the orthodontist one bracket at a time or can be done all at once with a jig or matrix that has the brackets pre-placed (i.e. indirect bonding). I use both systems in my office.
To adhere the bracket to the tooth, the tooth is first cleaned and conditioned with an etching material. Etching is done to create micrporosities in the enamel that can only be seen with an electron microscope. These microporosities allow little micromechanical locks for the thin resin bonding agents to be applied to the tooth. The tooth is now chemically prepared to adhere to the bracket with a composite resin paste that is applied to the back of the bracket and then placed on the prepared tooth. LED light is then used to set the polymers in the adhesive paste and harden the resin to attach the bracket to the tooth. This resin paste is the same as the tooth colored material used for fillings.
The bonding process of the teeth is reversible. Braces have to be taken off at the end of treatment. And when braces are removed, they are clicked off with use of an orthodontic plier and the mechanical bond between the tooth and brace is broken. Now if that bond were too strong, the enamel of the tooth would be damaged. So the bond strength is designed to be weak enough that the braces can be “broken off” without damaging the tooth.
Like any other adhesive, applying excessive force can sheer off the bond and result in detachment of brackets from the tooth surface. That is why, your orthodontist recommends avoiding certain food during your orthodontic treatment. Any food that is too hard, too chewy, or too sticky can compromise the bonding of the resin and detach your brackets from your teeth. Foods that are hard can impart enough pressure to give the energy to break the bond between brace and tooth. So, before you bite into anything, think about weather or not it would break the bond of brackets with your teeth. If the answer is yes, cut your food into pieces before eating or simply avoid eating them until your treatment is completed. Re-bonding the broken bracket is simple. However, broken brackets disturb the balance designed in the system of braces and archwires and can create undesirable movements or delay tooth movement.
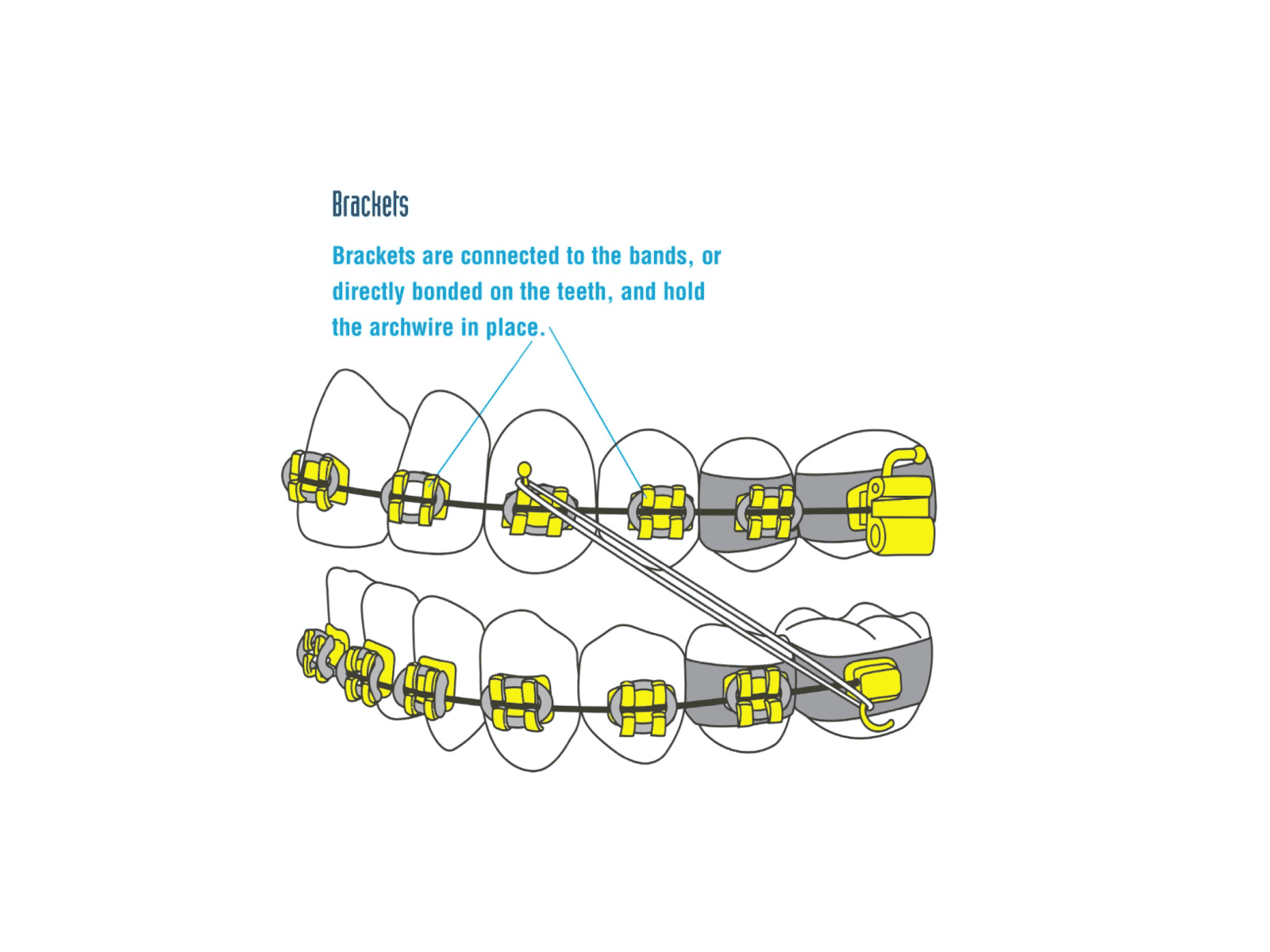
Brackets are generally bonded to the labial (front side) of the teeth using a resin based dental adhesive.
Brackets serve as handles to hold the wire in place and insert the force of the wires to the teeth.
Today’s brackets are small and sleek, especially compared to brackets of a generation ago– or even those from 10 or 15 years ago. Probably most of the brackets you will see will be made of stainless steel. But some patients opt for ceramic brackets. Some may even have gold-plated brackets.
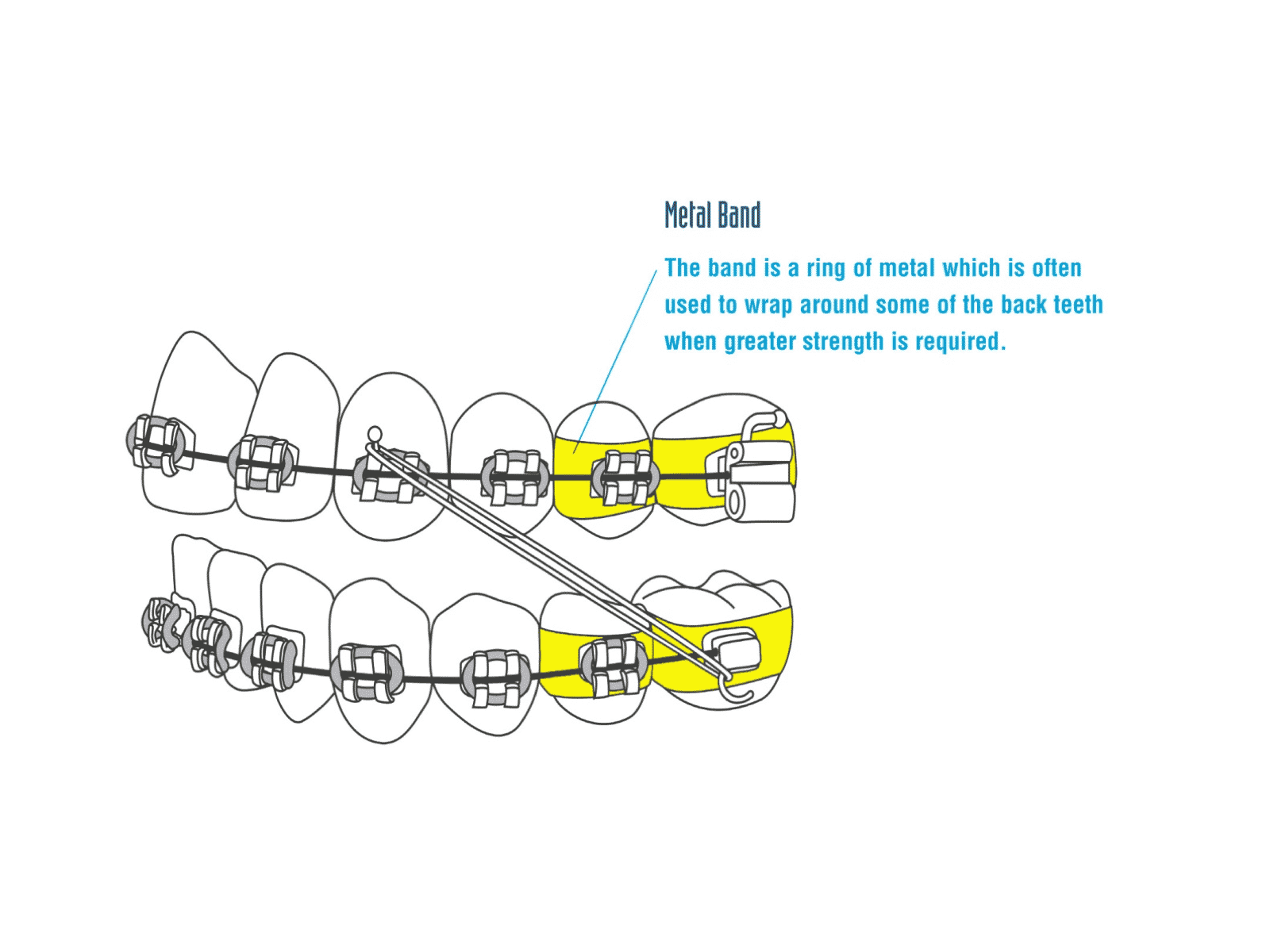
The “band” is a metal ring that wraps around a tooth – usually a molar – to provide an end point for insertion of the wire. The band is cemented to help it stay in place for the duration of treatment. Bands can also be used as part of orthodontic appliances such as expanders.
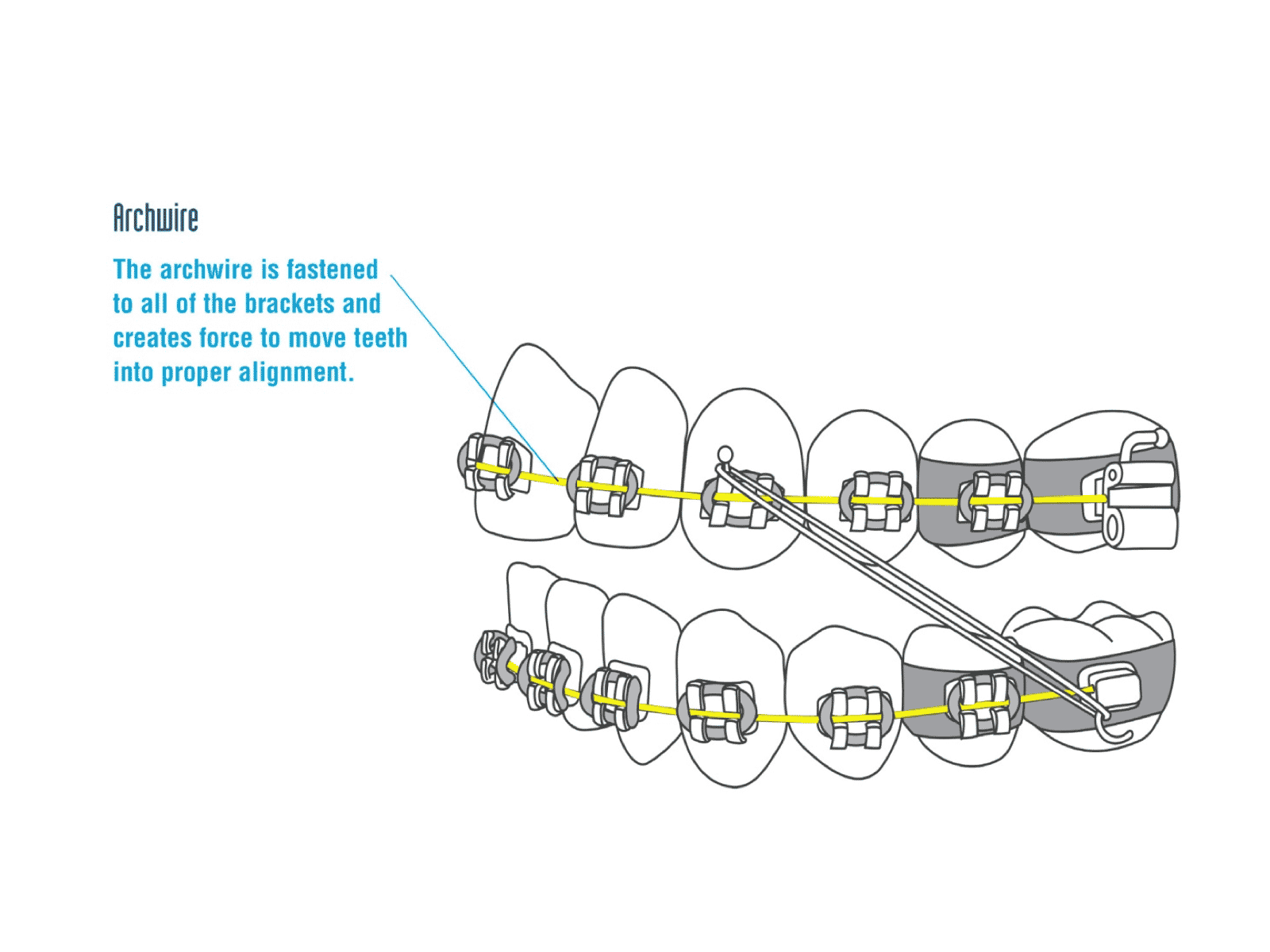
The archwire, or wire, fits in the horizontal slots in each bracket. The wire is secured to all of the brackets as discussed previously.
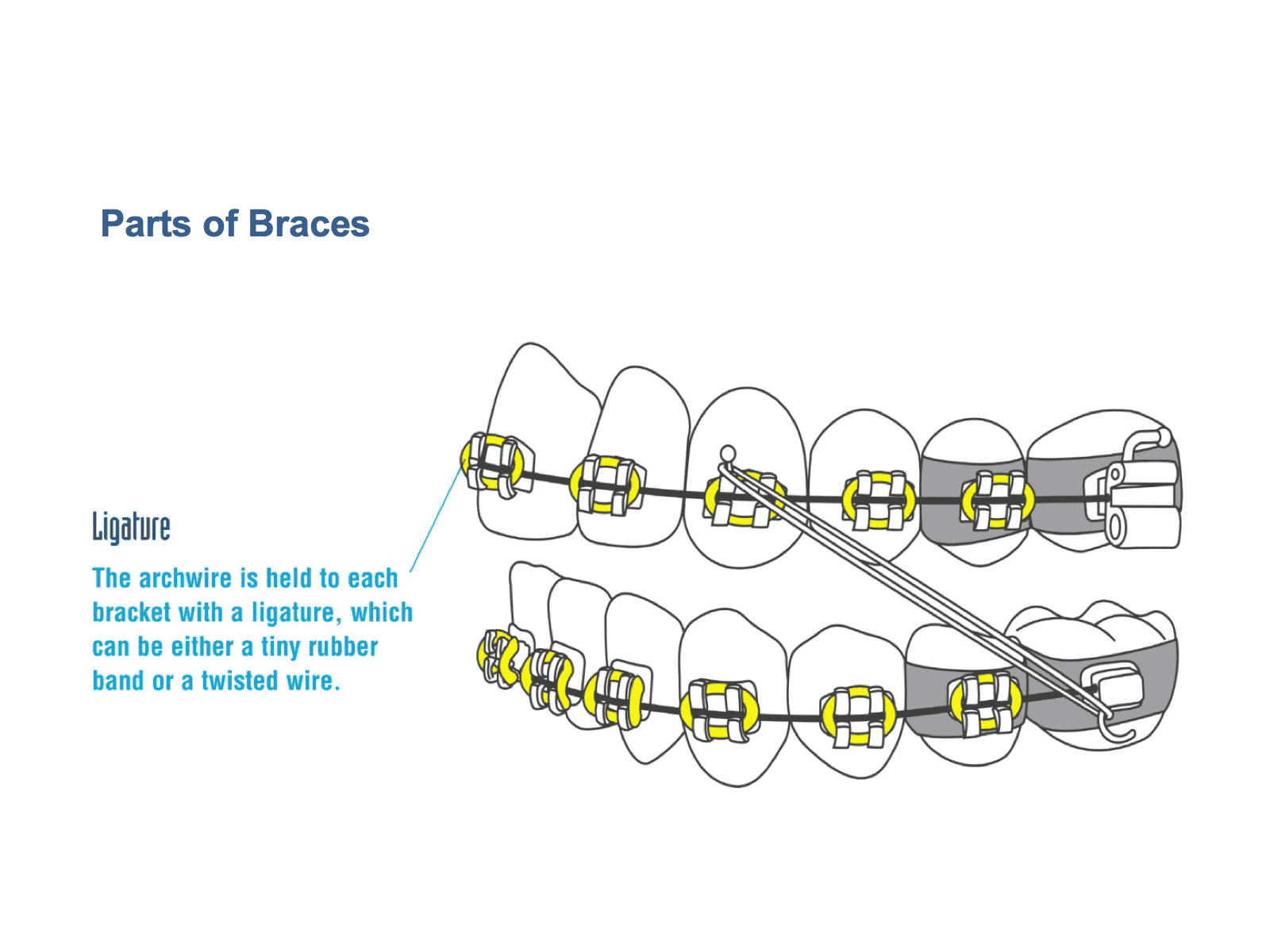
Ligature is a tiny rubber band or a metal tie that is stretched around the bracket. It holds the wire in the slot of the bracket so that it can deliver force to the teeth and move them.
Patients often select fun colors for their rubber ligatures. The ligatures are changed at each adjustment appointment.
Sometimes a twisted wire is used instead of a rubber ligature. There are some braces that don’t use ligatures at all. Those are called “self-ligating” braces. They have their own built-in method of holding the wire to the brackets.
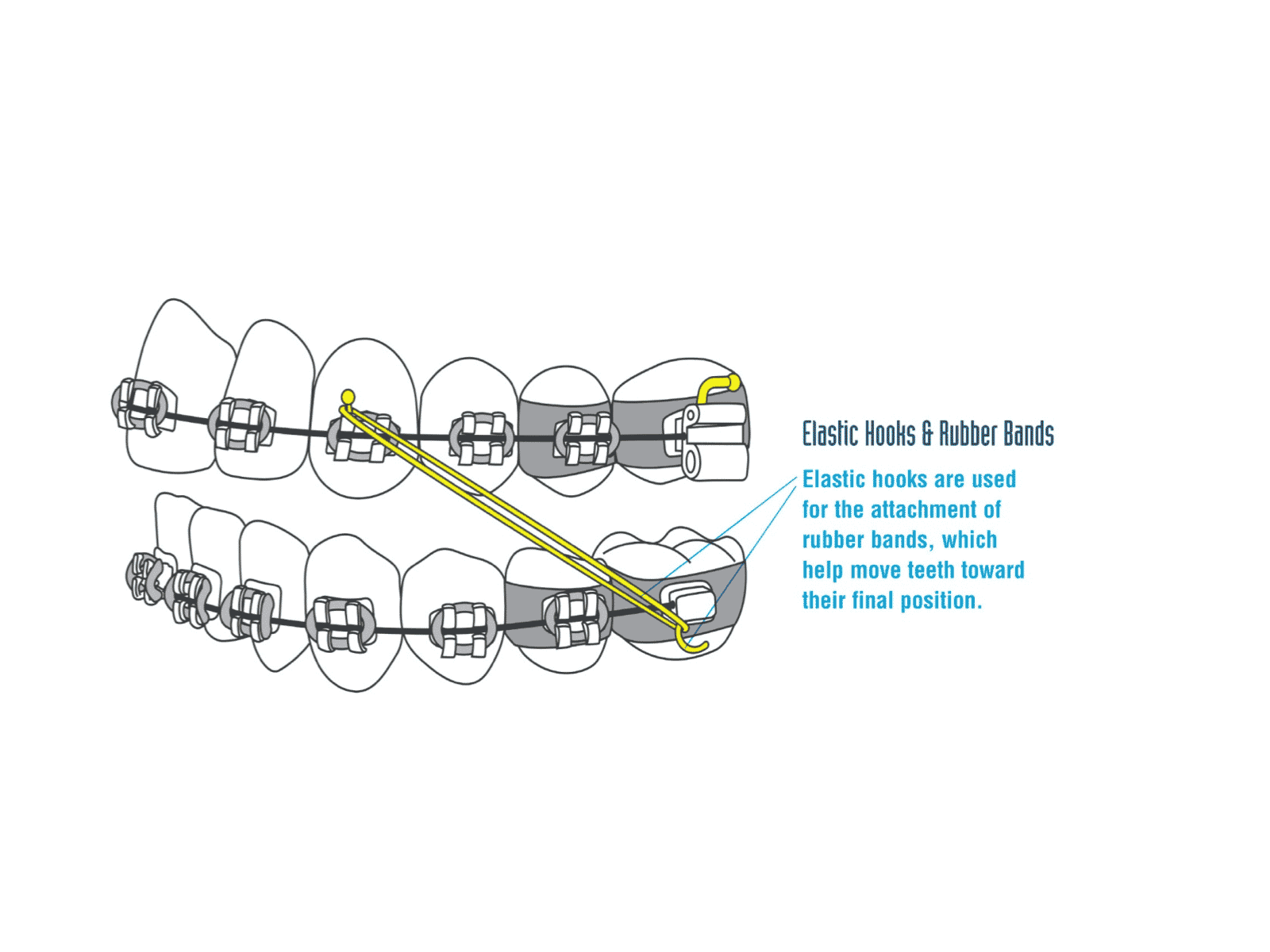
Elastic hooks are used to attach rubber bands.
These are the rubber bands that patients put in and take out themselves. They are often prescribed to help move the teeth toward their final positions and to align the bite. Wires alone cannot always move teeth where they need to go or bring the bite into its final alignment. Rubber bands will not necessarily be prescribed for every patient. However, when prescribed, your cooperation with your orthodontist recommendation is essential in order to achieve ideal treatment outcome.
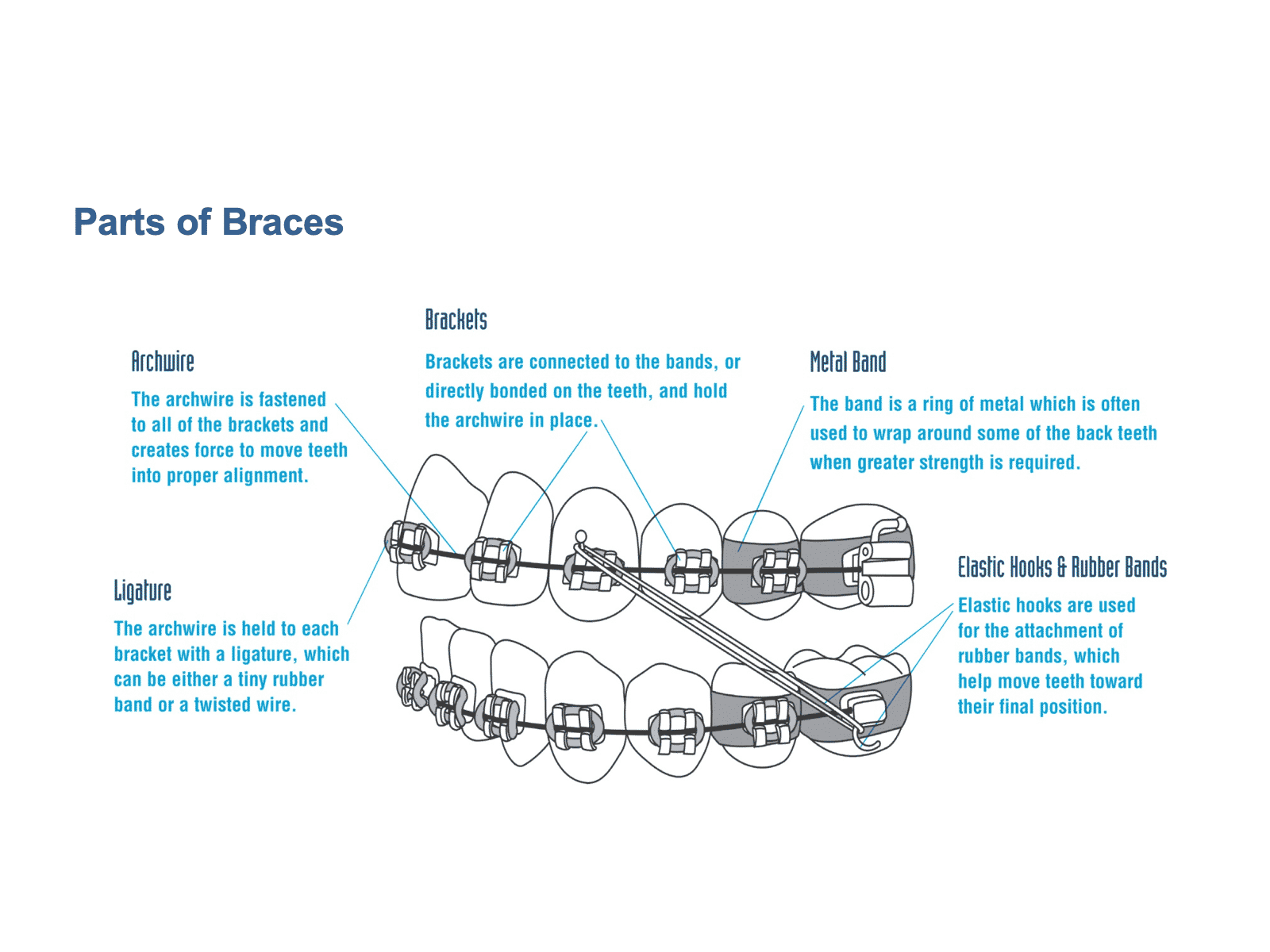
So putting it all back together, here are all of the components that can make up a set of braces.
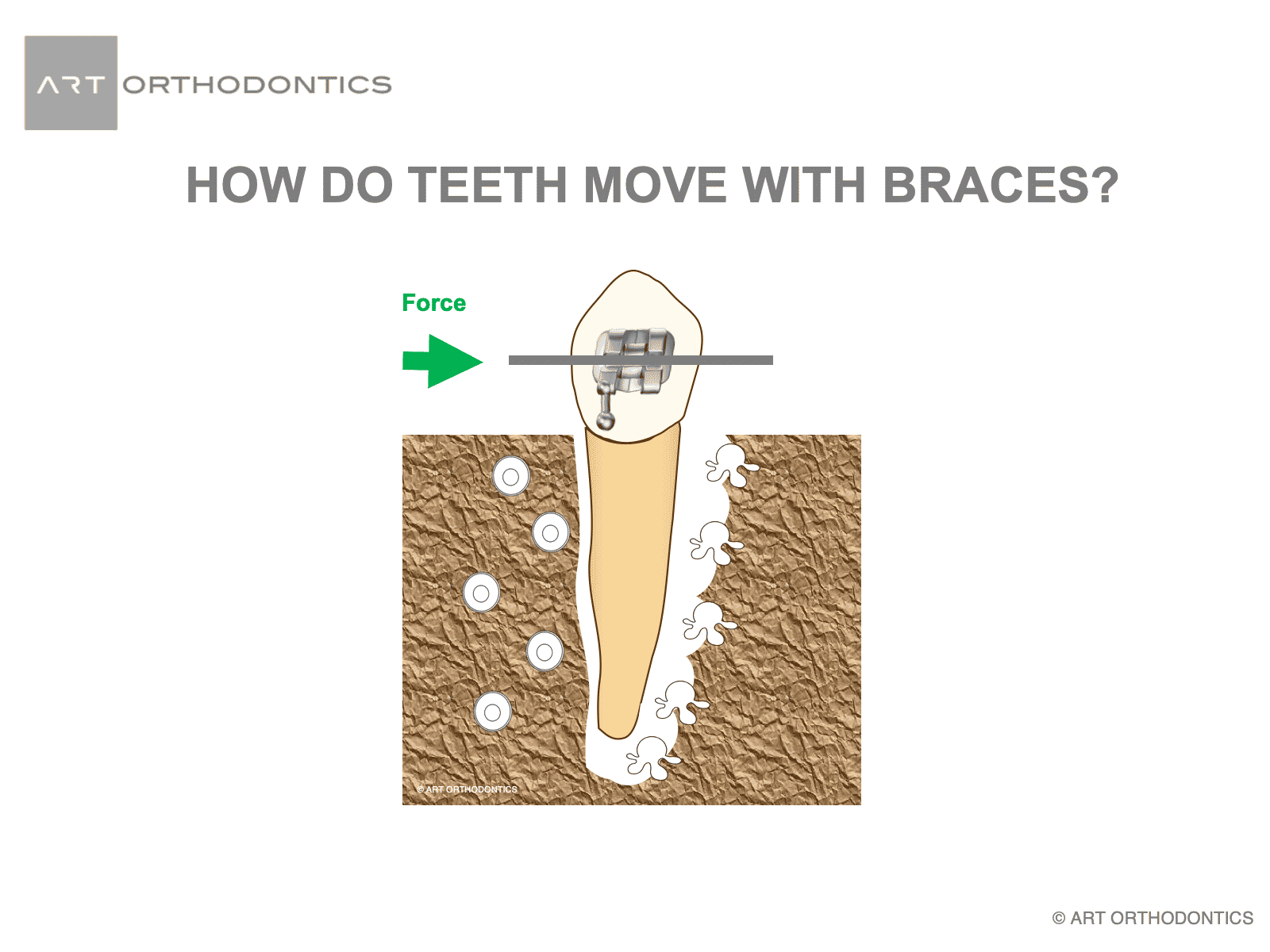
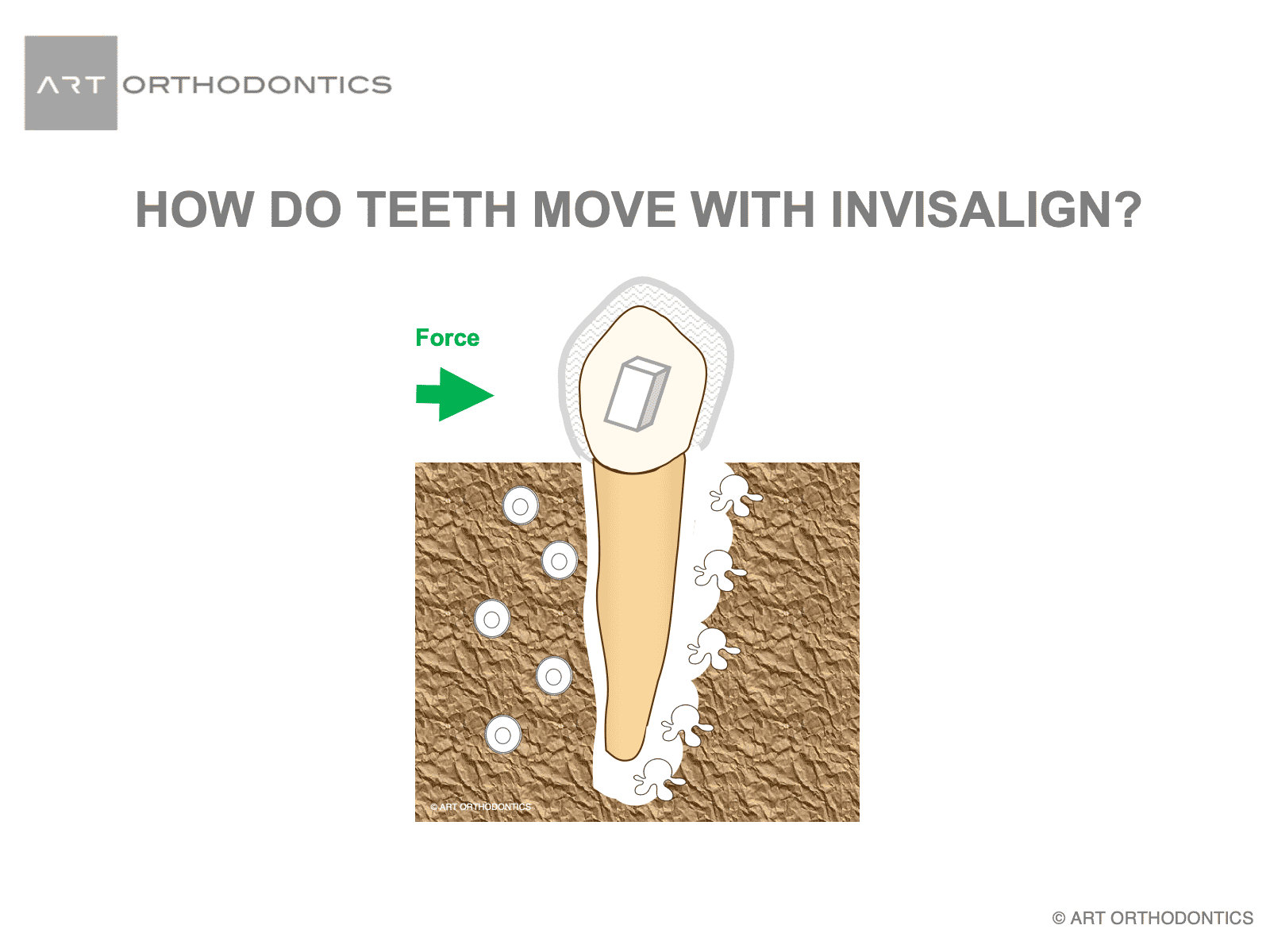
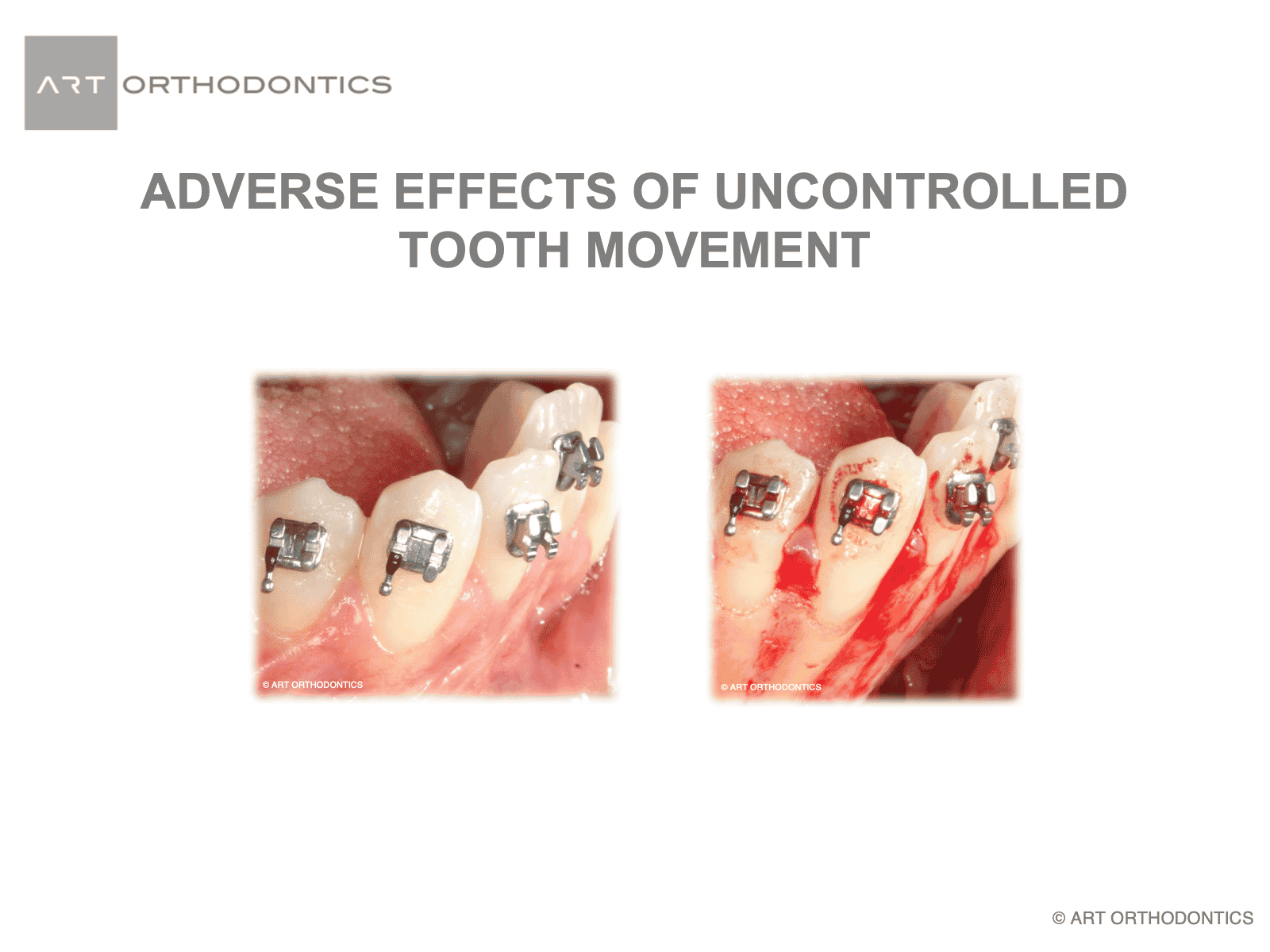
Placement of wires into brackets leads to application of pressure to the teeth and surrounding tissues. This pressure will result in resorption (dissolving) of the bone around the tooth. Once the tooth is in its new position, new bone is formed around the tooth to maintain it. The direction and amount of the forces applied to teeth is determined by your orthodontist and should be closely monitored to prevent adverse effects such as resorption of the roots of teeth or bone.
Insertion of aligners applies pressure to the teeth. This pressure will result in resorption (dissolving) of the bone around the tooth. Once the tooth is in its new position, new bone is formed around the tooth to maintain it. The design of resin attachments bonded to your teeth, and direction of forces applied to them are determined by your orthodontist and should be closely monitored to prevent adverse effects such as resorption of the roots of teeth or bone.
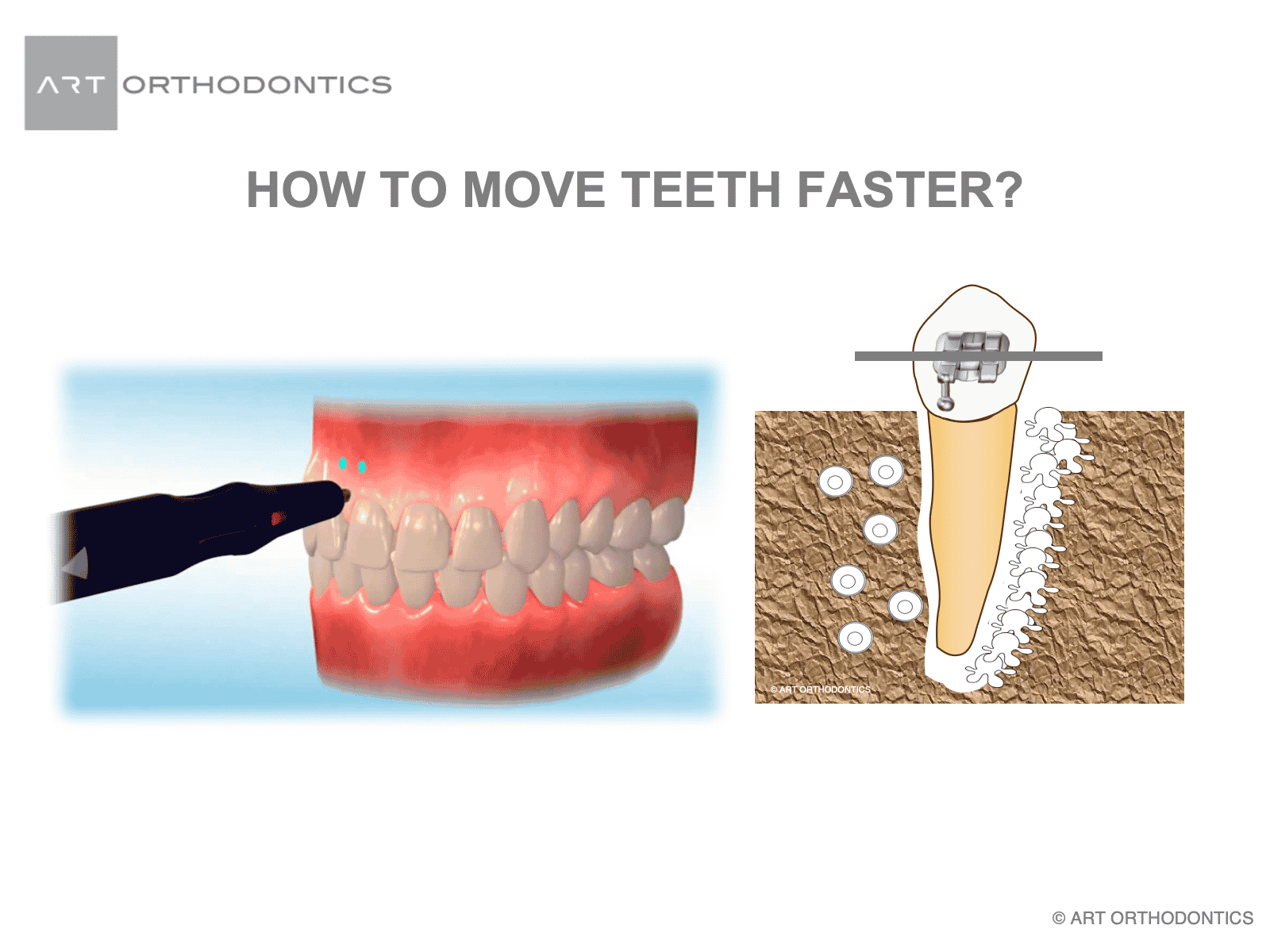
Microosteoperforation is a procedure whereby small perforations are made in the bone surrounding the tooth to expedite its movement. This procedure recruits the cells involve in the process of remodeling the bone around the tooth.
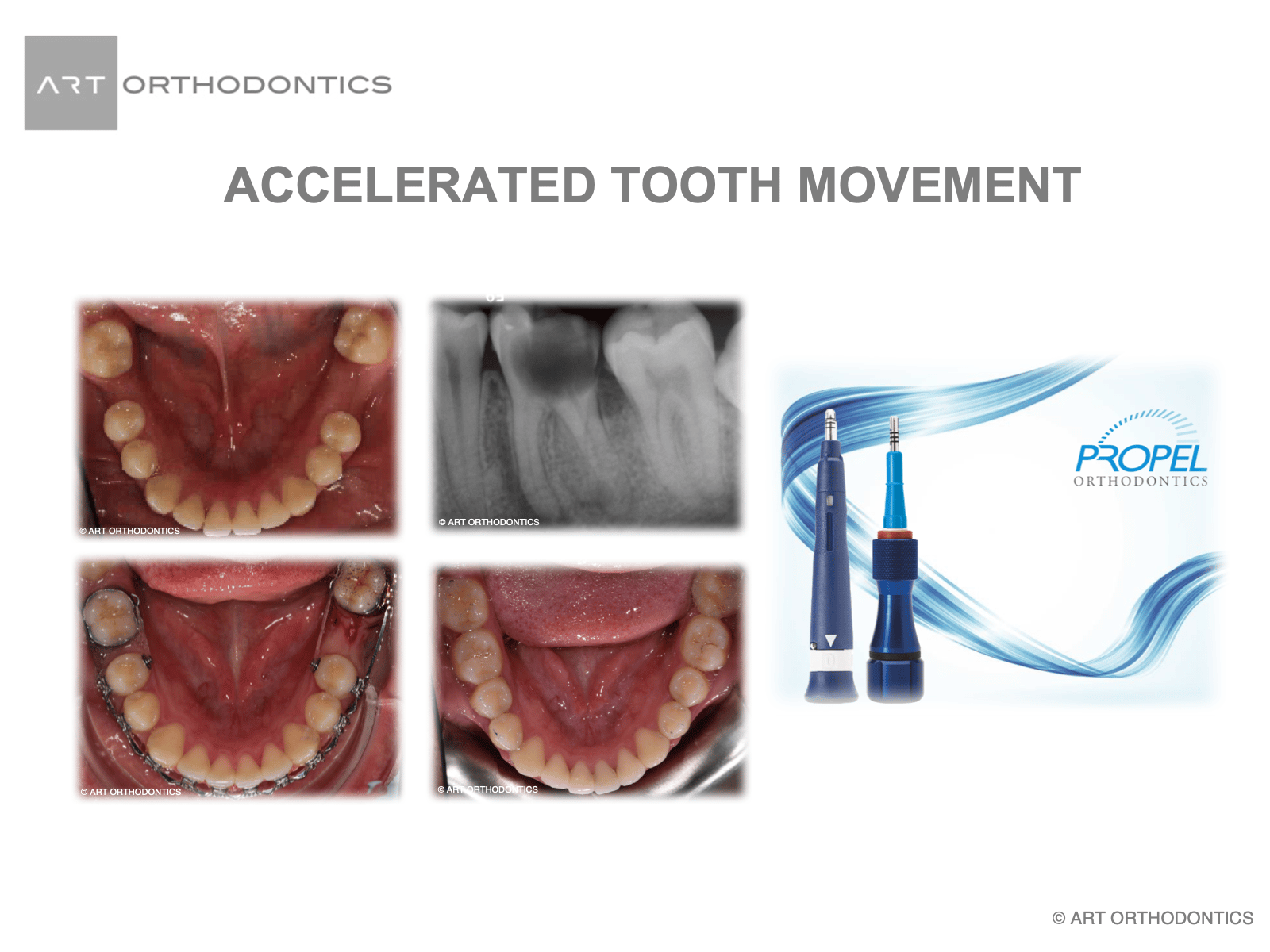
Dr. Khatami has been mentoring orthodontic residents and conducting several studies at Nova Southeastern University to explore which technique of accelerating tooth movement works best to produce healthier and faster outcome.
Use of Propel device and microosteoperforation accelerated movement of the second molar to replace the missing first molar.
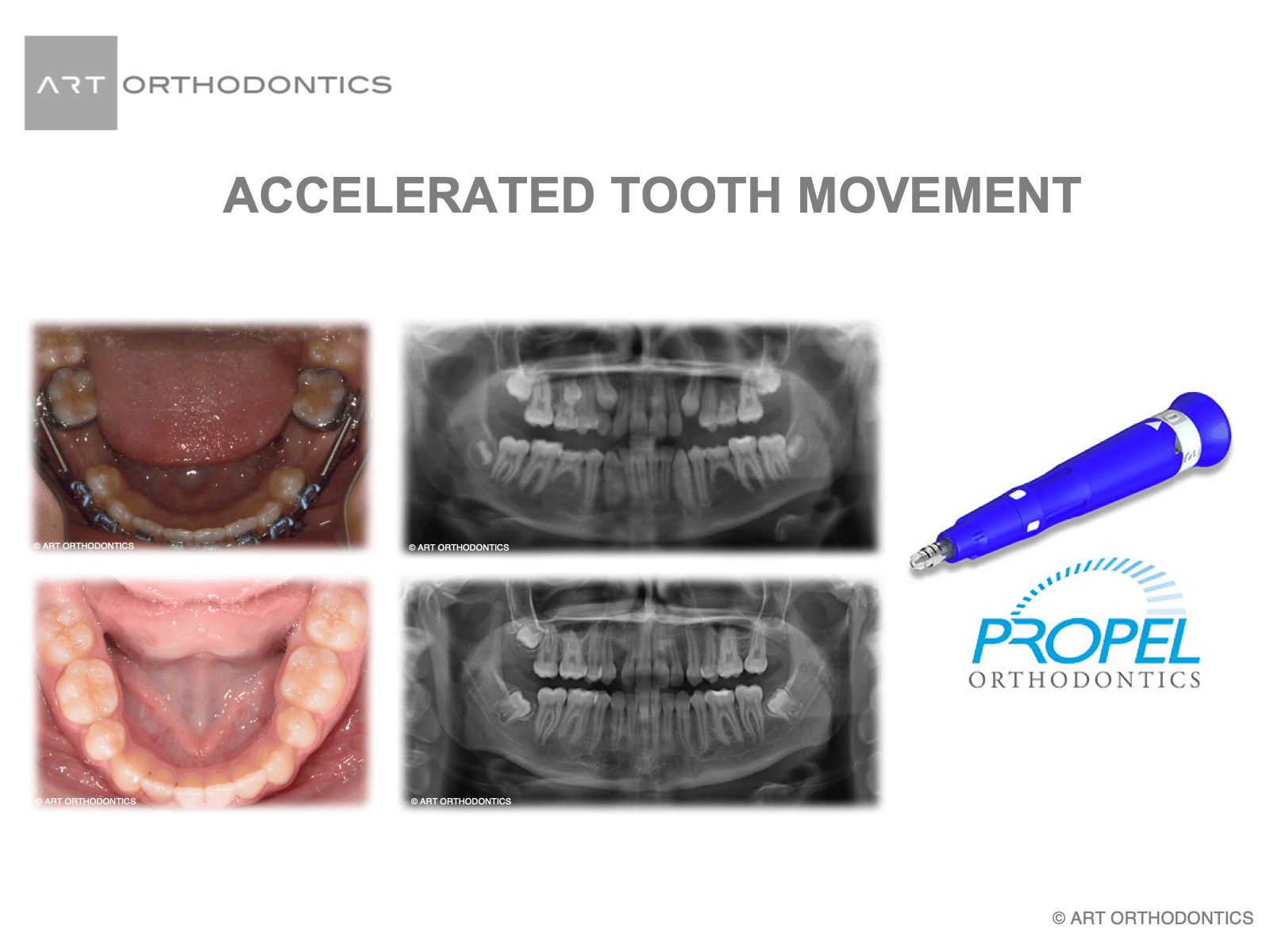
Here is the before and after images of using the propel system and braces to accelerate tooth movement of the first and second molars forwards. The propel system also helps in the direction of movement to move the back teeth forwards, versus the front teeth back. This is a huge benefit to treatment and you can see the extra space for the third molars.
If teeth are moved too far beyond the biological limits of their surrounding tissues, the surrounding bone will resorb. Teeth will lose their support, may get loose, and eventually lost. Your orthodontist evaluates the amount of bone available and discuss options such as extractions to maintain your teeth within healthy bone while they are moved into ideal position.
I hope that this section of the ART Orthodontic Blog has been informative and educational. It is important to understand that there are many factors that go in to orthodontic treatment. It is not only about making a beautiful smile. It is important to understand the basic tenants of biology and physiology and to know how and where to move the teeth. It is also important to understand the mechanics and engineering involved in moving the teeth. I am proud of my training and background and my mentor Dr Subtelny was a pioneer in orthodontics early in his orthodontic career and he was a leader his whole career. He lead by example and he lead by making all of his students think and to understand that in orthodontics – the “root is the root of the problem”.
This means that the person moving your teeth needs to have an understanding of the biology, the anatomy, the physiology, and the mechanics of braces to properly align the teeth and their roots to have a successful result that is stable long-term and healthy for the gums and bones.
Coupling this series of slides with the previous set of slides hopefully provides and understanding of the complexity involved in orthodontic treatment and gives you confidence in seeking treatment at ART Orthodontics where we will use our training and expertise to give you the best results possible that will last your lifetime.